

Dr. Sujith Mathew Issac, MS ( Ortho ), MRCS ( EDIN, UK )
Fellowship in Arthroscopy and Sports medicine
Arthroscopy and Sports medicine Specialist

Recurrent Dislocation of Shoulder
RECURRENT DISLOCATION OF SHOULDER
The shoulder joint consists of a ball (humeral head) and socket (glenoid). The ball is held in its place in the socket by a cartilage rim around the socket (labrum) and ligaments which attach to the ball on one side and to the socket on the other.
RECURRENT DISLOCATION means the ball of the shoulder joint repeatedly gets displaced from its original position. This usually occurs towards the front of the socket (anterior dislocation).
THERE ARE TWO TYPES OF DISLOCATIONS :
- Dislocations following injury (trauma) :
- Dislocations due to lax ligamnents :
Dislocations following injury (trauma) follows a fall or violent trauma to the shoulder as in contact sports. Here, the ligaments and labrum are torn off the edge of the socket (Bankart lesion).It usually results in a defect in the ball (humeral head) as well ( called a Hill-Sachs lesion).Sometimes, particulary following multiple dislocations, the bone of the socket can be get eroded or pulled off along with the ligaments.
Dislocations due to lax ligamnents occur with minor trauma or sometimes,none at all. This is usually associated with shoulder dislocations in different directions (Multi -Directional Instability). These patients usually have laxity in their other joints as well.
DIAGNOSIS
- Clinical : A complete dislocation is very painful and disabling and the patient will not be able to move his limb at all. There will be a loss of “roundness” of his shoulder.After reduction of the dislocation, the pain comes down significantly.There can also be partial dislocations (subluxation) which are not that extremely painful and may be associated with only mild pain on certain positions of the shoulder.Neverthless, even these repeated subluxations can damage the joint in the long term.
- X-Ray : The dislocation can be usually,easily diagnosed on an x-ray.
- Ultrasound : It is also used to confirm the reduction of the dislocation
- MRI : This is not required in every case.MRI is mainly used in Recurrent Dislocation to diagnose a Bankarts lesion and any other ligament abnormalities in the shoulder,while planning a surgical treatment
- COMPUTER TOMOGRAPHY (CT) SCAN : This is done to assess the degree of bone loss on the glenoid as well as humeral headThis is crucial for decision making as to which surgical procedure is ideal for the given patient.For this, a 3D reconstructed image of the glenoid and humeral head are made and certain measurements done using a computer software
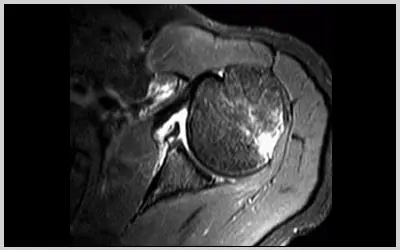
MAGNETIC RESONANCE IMAGING (MRI)
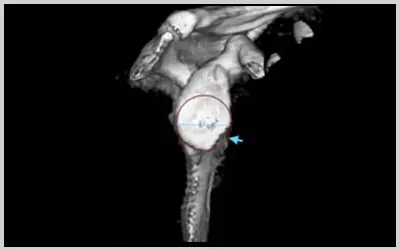
3D Reconstrution of the glenoid bone showing bone loss (Blue arrow)
TREATMENT
Following the first dislocation, after reduction, usually the limb is kept in a sling for 3-4 weeks. This is to give the torn ligaments a chance to heal. The healing depends on factors like age of the patient ; the younger the patient ,the lesser the chance of the ligament to heal back. If the ligament doesn’t heal in a few weeks, then the patient runs the risk of repeated dislocations.With each repeated dislocation, the shoulder joint is progressively more damaged and the bone loss becomes more marked.
Injuries associated with repeated dislocations, like rotator cuff tears, fractures ..etc are more common when dislcoations occur in older patients.Dislocations due to ligament laxity can usually be treated successfully with physiotherapy.Surgery is required only if conservative treatment fails.
DIFFERENT SURGERIES AVAILABLE FOR RECURRENT DISLOCATION OF SHOULDER :
Arthroscpic Bankarts Repair :
This is an arthroscopic procedure (key-hole surgery) where the torn ligaments (Bankart lesion) are repaired back to the bone (glenoid).
Here, three small holes (portals) are made (measuring a few millimetres) around the shoulder joint and instruments passed through them to do the surgery.First, the bone (glenoid) is prepared and then suture anchors ( which get converted to bone in due course of time ) are inserted into it.
Suture Anchors are tiny devices with sutures or threads attached. Using the sutures attached to the anchors ,the ligaments are repaired back to the glenoid.

Arthroscpic Bankarts Repair :

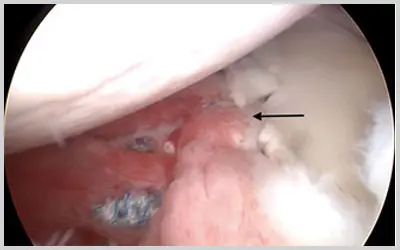
Arthroscpic View of the shoulder before repair :
Black arrow – labrum (along with ligament) torn from the bone (Bankart lesion)
White arrow – bone (glenoid)
Arthroscpic View of the shoulder after the Bankart repair :
Black arrow – labrum repaired back to the bone (glenoid)
See Surgical videos section for a video clip of the procedure
Arthroscopic Remplissage Procedure
This is performed along with the Arthroscopic Bankart Repair when there is a large bone loss in the ball of the shoulder joint (humeral head) called a Hill-Sachs Lesion.
Here, the defect in the humeral head is filled in with a rotator cuff muscle.

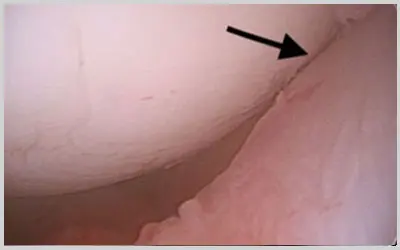
Arthroscopic view of the humeral head defect (Hill-Sachs Lesion) (Black arrow)
Arthroscopic view of the humeral head defect filled in with muscle (Black arrow)
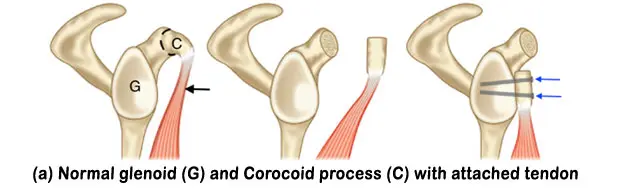
Latarjet Procedure
This is done when there is a large bone loss from the glenoid bone.When the bone loss is small, a Bankart procedure may suffice. To accurately determine the bone loss and to determine whether a Latarjet procedure is required, certain calculations have to be done from the patient’s CT Scan.
In a Latarjet Procedure, a small bony extension seen adjacent to the shoulder joint, called the corocoid process, is cut from its base along with a strong tendon attached to it, and screwed onto the defect in the glenoid.This bone along with its attached tendon prevents any further dislocation of the shoulder.This is a highly successful surgery but is indicated only in few cases.It is particularly good for contact athletes , who wish to return to their previous perfomance level.
POST OPERATIVE REHABILITATION
HOSPITAL STAY is short; usually one or two days
During this period,the operated arm should not be lifted for any activities.The elbow and wrist need to be moved periodically. We will educate you on the other specific excercises that need to be done during this period;these may be done at home itself.
FIRST 6 WEEKS
- THE OPERATED ARM WILL BE PUT ON A SLING FOR 6 WEEKS. It may be removed at home in a protected environment, for some time and for actively moving the elbow, wrist and fingers with the arm by the side of the body. Sling has to be definitely worn at night and while going out.
- Driving is not allowed for 6 weeks
- Sleeping on the affected shoulder also will be difficult.
- Daily activities like brushing teeth & shaving may be done with care ; but all activities causing extreme rotations of the arm are not allowed. You will be briefed about these after the surgery.
- Office work like working on a computer and writing may be done.
6 WEEKS TO 12 WEEKS
- Sling is discontinued.
- THE ARM IS ALLOWED TO BE MOVED ACTIVELY AT THIS TIME.
- Driving is also allowed
- SPECIFIC STRECTCHING AND STRENGTHENING EXCERCISES ARE STARTED. OUR PHYSIOTHERAPIST WILL SUPERVISE THESE INITIALLY, WHICH CAN BE CONTINUED AT HOME.
AT 4 MONTHS
- At this time, the patient can begin working out in a gymn.
- FULL UNRESTRICTED ACTIVITIES ARE ALLOWED FROM 6 MONTHS.
SUCCESS RATE
- The above described surgeries for recurrent dislocation of the shoulder are highly successful in stabilizing the shoulder.
- But the critical points are to ascertain the specific procedure required for a particular patient and the surgical expertise to perform them adequately.